
Organic
Impotence:
Vascular
Abnormalities
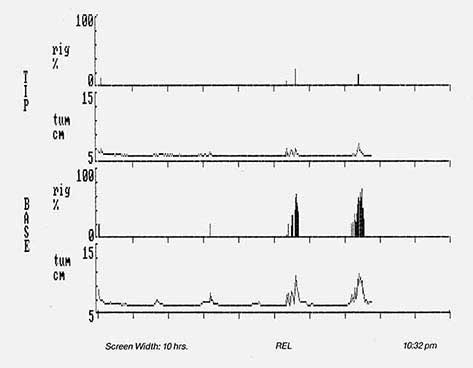
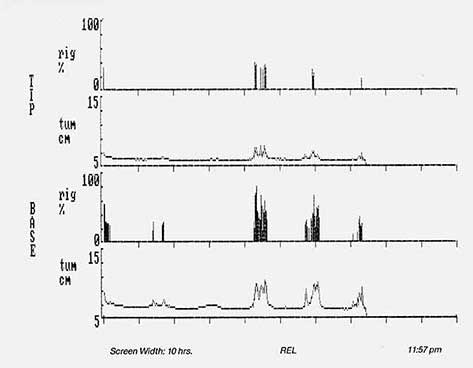
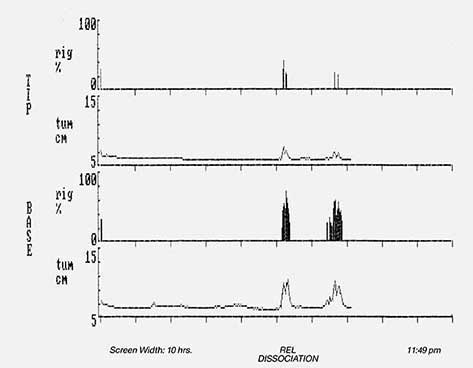
Patient Identification: REL
General Medical Hx
retired widower, 6 children
age: 61
med.dx : HTN, diagnosed 1975
spinal arthritis
surgeries: C5, C6 disk, 1967
C4, C5 disk, 1970
smoker: no
alcohol: 6 oz. wine/day x many years
meds: Hygroton, 25my. q. d.
Sexual Hx
• difficulty obtaining and maintaining erections since 1975
• complain of penile numbness
• gradual onset of sexual dysfunction
• occasional A.M. erections, denies nocturnal erections
• slight improvement of erection with masturbation and in supine position
upon awakening
• penile curvature: denies
• last successful intercourse: 1979-1980
• ejaculation intact – masturbation
• premature ejaculation: denies
• libido: normal
• bladder symptoms: denies
• bowel symptoms: denies
• sleep disturbances: considers himself a restless sleeper ( arthritic pain
awakens him 3-4 times/night)
Physical Exam
WNL except it. Kidney palpated
BP: 170/80
Test Results
Glucose, TST—WNL
Doppler
Rt.
Lt.
Mid
Pre-Exercise (PBI)
.80 – NI.
.79 – NI.
.73 – Borderline Abnl.
Post-Exercise (PBI)
.71 – Borderline Abnl.
.70 – Borderline Abnl.
.55 – Abnl.
Electrophysiological Tests
NCV of DNP
PER
BCR
42 M/sec/ - NI.
not ordered
not ordered
RigiScan: Abnl. X 3 nights – DISSOCIATION (distal penile shaft softening)
Final Dx
Organic impotence associated with vascular insufficiency
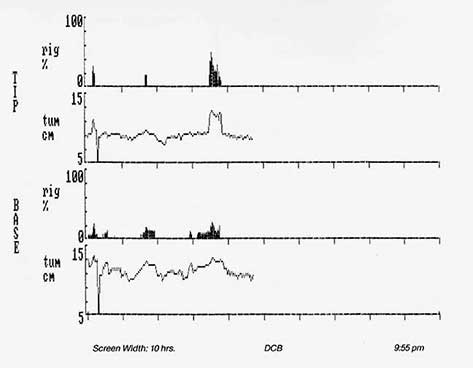
Patient Identification: DCB
General Medical Hx
assistant with gas and electric company, single, 0 children
age: 25
med. dx: blunt trauma to groin area (right testicle and penis by wire
cable on 5/85)
surgeries: eye surgery as a child
repair of corpora cav. Venous shunts on 9/85
smoker: 1/2 pack per day
alcohol: occasional drink
meds.: none
Sexual Hx
- difficulty obtaining and maintaining erections since injury 5/85 and right testicle pain
- denies decrease of penile sensation
- rapid onset of sexual dysfunction
- semi A.M. erections since 5/85
- minimal improvement of erection with other types of sexual stimuli
- penile curvature: denies
- last successful intercourse: 3 weeks ago, used stuffing technique
- ejaculation intact –intercourse 3 weeks ago
- premature ejaculation: denies
- libido: normal
- bladder symptoms: denies
- bowel symptoms: denies
- sleep disturbances: denies
Physical Exam
WNL except it. varicocele
Test Results
Glucose, TST, Prolactin, LH – WNL
Doppler
Rt.
Lt.
Mid
Pre-Exercise (PBI)
.98 – NI.
.91 – NI.
1.00 – NI.
Post-Exercise (PBI)
.72 – Borderline Abnl.
.75 – NI.
.75 – NI.
Electrophysiological Tests
NCV of DNP
PER
BCR
40 M/sec/ - NI.
not ordered
not ordered
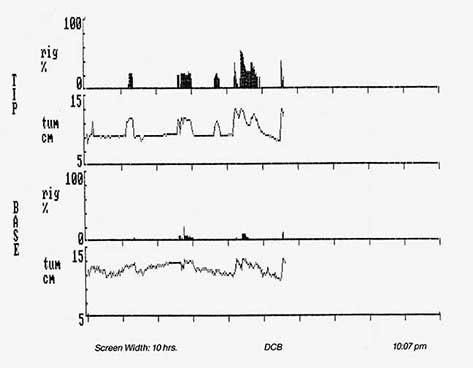
RigiScan: Abnl. X 2 nights – abnormal tumescence and rigidity of penile shaft ( base greater than tip)
Penile Arteriogram: WNL
Corpora Cavernosagram: presence of venous shunts
Final DX
- vasculogenic impotence secondary to venous leakage
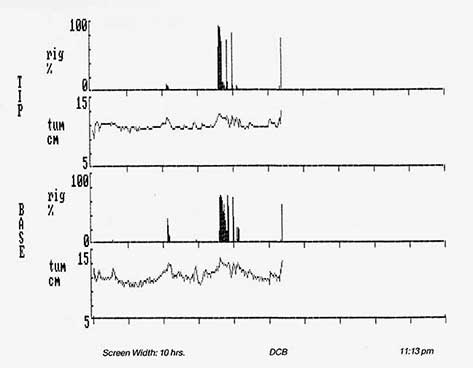
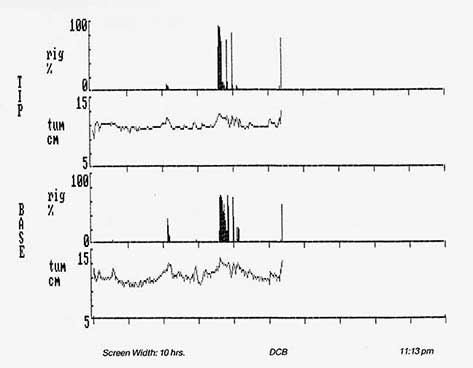
- 9/85 surgical repair of corpora cavernousus venous shunts.
- RigiScan:post-op x 3 night—normal rigidity of base and tip penile shaft
- average base rigidity was in the 70-75% range
- average tip rigidity was in the 90-95% range
- patient states he is having successful intercourse with firm erections
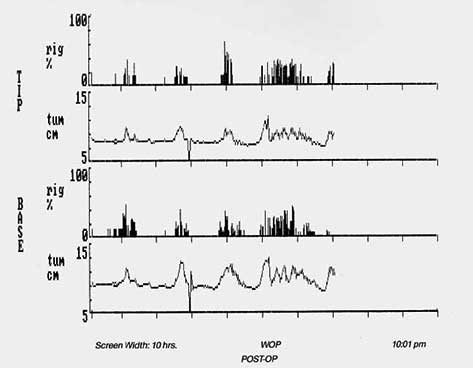
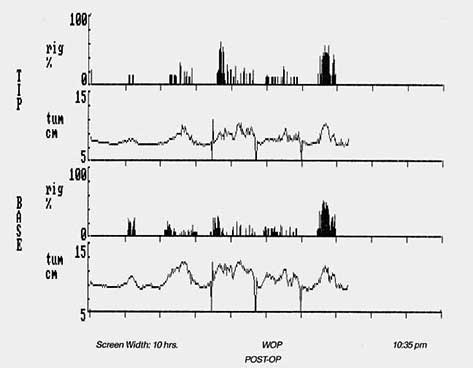
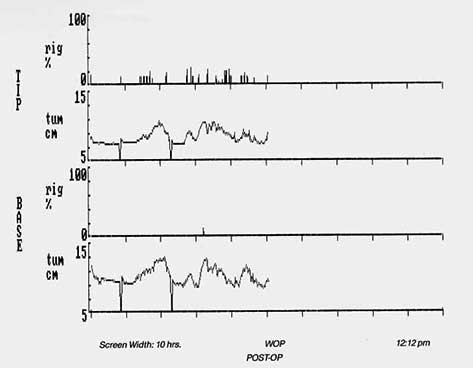
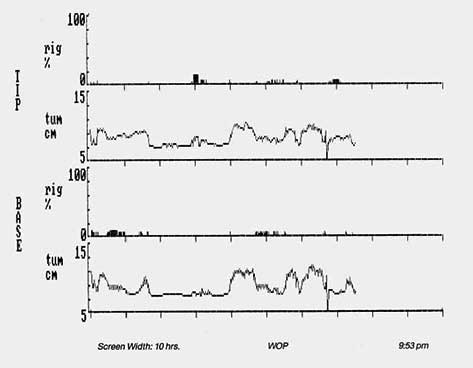
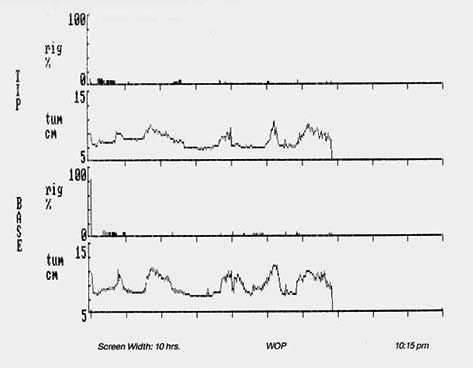
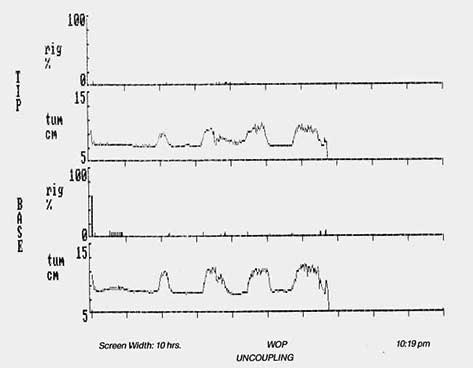
Patient Identification: WOP
General Medical Hx
handyman, married x 2 (#1-12 years, divorce: #2-32years, wife deceased April,
1985 of cancer), 1 child
age : 64
med. dx: none
surgeries: Hydrocele, 1939
repair of corpora cav. Venous shunts on 9/85
smoker: no
alcohol: none
meds.: none
Sexual Hx
- difficulty obtaining and maintaining erections since June, 1985
- complains of decreased penile sensation
- gradual onset of sexual dysfunction
- occasional semi A.M. and nocturnal erections
- has not used other types of stimuli to evoke erections ( masturbation,
- oral sex or erotic films)
- erections are not sufficient for vaginal penetration
- does not notice any improvement in erections with position changes
- penile curvature: denies
- ejaculation intact during last successful intercourse
- complains of premature ejaculation when last attempted sex
- libido: normal
- has received testosterone injections and pills in the past which were unsuccessful in improving erections
- bladder symptoms: denies, except for difficulty starting stream on occasions
- bowel symptoms: denies
- sleep disturbances: denies
Physical Exam
essentially WNL
BP: 130/90
Test Results
Glucose, TST, Prolactin, LH – WNL
Doppler
Rt.
Lt.
Mid
Pre-Exercise (PBI)
.97 – NI
1.00 – NI
absent
Post-Exercise (PBI)
.91 – NI
1.00 – NI
absent
Electrophysiological Tests
NCV of DNP
PER
BCR
42 M/sec/ - NI
not ordered
not ordered
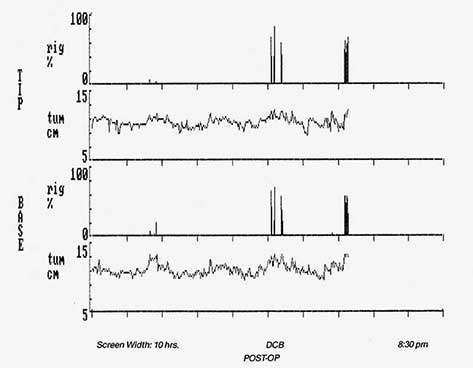
RigiScan: Abnl. X 3 nights – UNCOUPLING ( nl. tumescence at base and tip of penile shaft with absent rigidity
Penile Arteriogram: NI
Corpora Cavernosagram: presence of venous shunts
Final DX
- Vasculogenic impotence secondary to venous leakage
- 9/85 surgical repair of corpora cavernosus venous shunts
- RigiScan: post-op x 3 nights – normal tumescence of base and tip of
- penile shaft with concurrent rigidity
- (20 --50% range of base and tip of penile shaft –abnl.)
- due to inadequate results, patient has subsequently had a penile prosthesis implanted
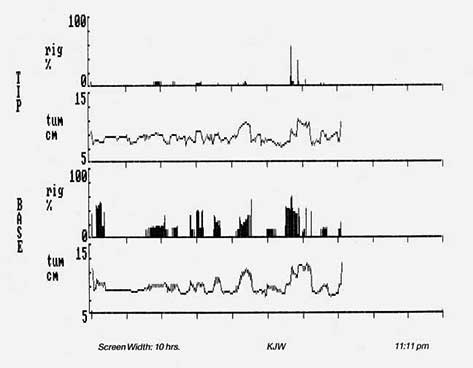
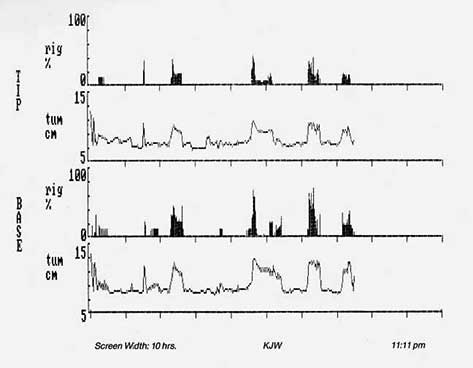
Patient Identification: KJW
General Medical Hx
self-employed, married x 28 years, 5 children
age : 52
med. dx: prostatitis in past
surgeries: none
smoker: no
alcohol: 1-2 beer or glasses of wine per day x many years
meds.: Depo-Testosterone 300 mg. I.M. 7/85 – 3/86
Sexual Hx
- difficulty obtaining and maintaining erections since 1980
- denies decreased penile sensation
- gradual onset of sexual dysfunction
- occasional semi A.M.and nocturnal erections
- no improvement with other forms of sexual stimuli
- erections are never sufficient for vaginal penetration
- no improvement in erections with position changes
- penile curvature: denies
- last successful intercourse: November, 1984
- ejaculation intact – oral sex
- complains of premature ejaculation
- libido: normal
- bladder symptoms: denies
- bowel symptoms: denies
- sleep disturbances: denies
Physical Exam
WNL
BP: not available
Test Results
Glucose, TST—WNL
Doppler
Rt.
Lt.
Mid
Pre-Exercise (PBI)
.72 – Borderline Abnl.
.93 – NI
.73 – Borderline Abnl.
Post-Exercise (PBI)
.72 – Borderline Abnl.
.75 – NI
.72 – Borderline Abnl.
Electrophysiological Tests
NCV of DNP
PER
BCR
42.8 M/sec. - NI
not ordered
not ordered
RigiScan: Abnl. X 2 night – UNCOUPLING (nl. tumescence at base and tip of penile shaft with reduced rigidity at base and tip of penile shaft) (tip greater than base)
Final DX
- organic impotence associated with vascular impairment
- SPECIAL NOTE: hormone injections have been ineffective in improving erections
RigiScan® is the registered trademark of GOTOP Medical, Inc., Copyright 2022 GOTOP Medical, Inc. All Rights Reserved.